Cardiovascular and autonomic activity responses after Active Cycle of Breathing Technique (ACBT) in healthy thais
Keywords:
Active cycle of breathing technique, Cardiovascular response, Autonomic activityAbstract
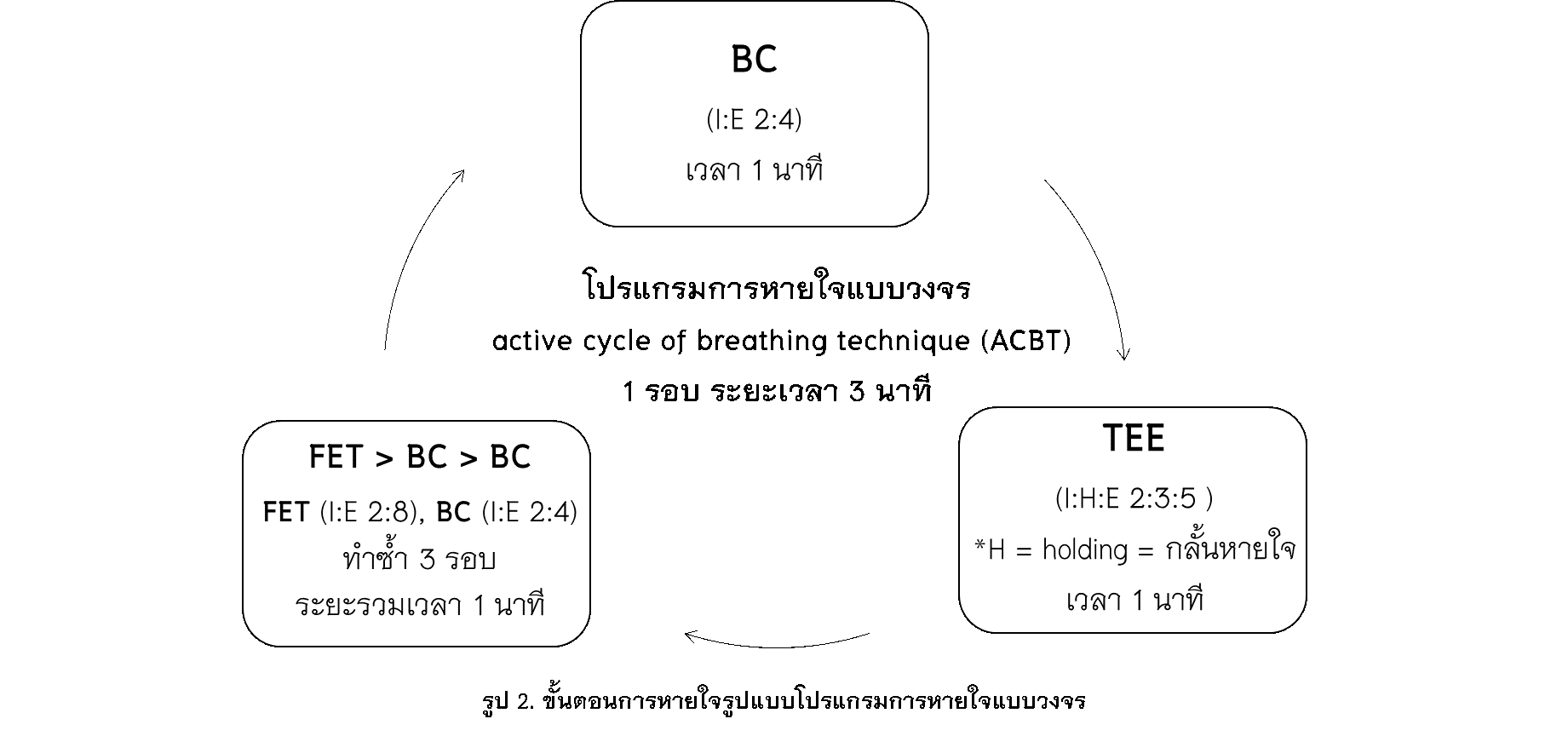
Currently, patients with respiratory conditions often had hypertension. The active cyclic breathing therapy (ACBT) technique is an effective technique for secretion clearance. Aim of this study was to clarify the physiological responses of the cardiovascular and autonomic nervous system activity after ACBT program. For safety reasons, it is necessary to understand the physiological response after ACBT program. Twenty subjects performed ACBT for 12 minutes and assessed cardiovascular response and autonomic activity before and after ACBT program. The results showed that ACBT affects systolic blood pressure (p <0.01), heart rate, oxygen saturation, and rate perceived exertion (p <0.05) was significantly increased. Moreover, significantly increased low frequency (LF) (p <0.05), and significantly reduced in high frequency (HF) and LF / HF. ratio (p <0.05) were observed after ACBT program. ACBT affects increased sympathetic activity leading to increased cardiovascular response. Treating respiratory patients with cardiovascular disease or abnormal autonomic activity with ACBT program should be careful.
References
Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789-858.
Vogelmeier CF, Román-Rodríguez M, Singh D, Han MK, Rodríguez-Roisin R, Ferguson GT. Goals of COPD treatment: Focus on symptoms and exacerbations. Respiratory Medicine. 2020;166:105938.
Lewis LK, Williams MT, Olds TS. The active cycle of breathing technique: A systematic review and meta-analysis. Respiratory Medicine. 2012;106(2):155-72.
Simpson J, Parsons N, Martin A. The role of the physiotherapist in paediatric respiratory medicine. Paediatrics and Child Health. 2019;29(4):178-84.
Lan C-C, Lai S-R, Chien J-Y. Nonpharmacological treatment for patients with nontuberculous mycobacterial lung disease. Journal of the Formosan Medical Association. 2020;119:S42-S50.
Battaglini D, Robba C, Caiffa S, Ball L, Brunetti I, Loconte M, et al. Chest physiotherapy: an important adjuvant in critically ill mechanically ventilated patients with COVID-19. Respiratory Physiology & Neurobiology. 2020:103529.
Nakanishi K, Takahira N, Sakamoto M, Yamaoka-Tojo M, Katagiri M, Kitagawa J. Effects of forced deep breathing on blood flow velocity in the femoral vein: Developing a new physical prophylaxis for deep vein thrombosis in patients with plaster cast immobilization of the lower limb. Thrombosis Research. 2018;162:53-9.
Pitzalis MV, Mastropasqua F, Massari F, Passantino A, Colombo R, Mannarini A, et al. Effect of respiratory rate on the relationships between RR interval and systolic blood pressure fluctuations: a frequency-dependent phenomenon. Cardiovascular Research. 1998;38(2):332-9.
Lehrer PM, Vaschillo E, Vaschillo B, Lu SE, Eckberg DL, Edelberg R, et al. Heart rate variability biofeedback increases baroreflex gain and peak expiratory flow. Psychosomatic Medicine. 2003;65(5):796-805.
Liu Y-W, Tzeng N-S, Yeh C-B, Kuo TBJ, Huang S-Y, Chang C-C, et al. Reduced cardiac autonomic response to deep breathing: A heritable vulnerability trait in patients with schizophrenia and their healthy first-degree relatives. Psychiatry Research. 2016;243:335-41.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2021 Naresuan Phayao Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยาไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย
The authors are themselves responsible for their contents. Signed articles may not always reflect the opinion of University of Phayao. The articles can be reproduced and reprinted, provided that permission is given by the authors and acknowledgement must be given.