Salivary pH, buffer capacity and total protein in saliva of dry mouth elderly patients
Keywords:
Salivary pH, Buffering capacity, Salivary protein, Xerostomia, Hyposalivation, ElderlyAbstract
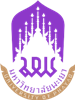
The objectives of this study was to analyze the relationship of salivary pH, buffer capacity and total protein in saliva of dry mouth elderly patients. Method: The subjects of this study were elderly patient (> 65 years old) 120 person. Divide into 4 groups by salivary flow rate measurement and xerostomia questionnaires, 1. Xerostomia and hyposalivation group, 2. Xerostomia group, 3. Hyposalivation group and 4. Normal group. All group were test pH by pH meter, Buffer capacity by Ericson’s method and Protein test by Biuret assay. Results: The results show that female elderly were had high prevalence of hyposalivation (53.75 %) than male (42.5%) and xerostomia (52.5 %) than male (40%). Salivary pH in normal group was higher than another groups. Buffer capacity were not significant different in each groups. Concentration of total protein in saliva for normal group had significant higher than xerostomia and hyposalivation groups. Conclusion: Xerostomia and hyposalivation group had significant different in salivary pH and salivary total protein.
References
Vissink, A., Spijkervet, F. K., & Van Nieuw Amerongen, A. Aging and saliva: a review of the literature. Spec Care Dentist, 1996; 16(3), 95-103.
Villa, A., Connell, C. L., & Abati, S. Diagnosis and management of xerostomia and hyposalivation. Ther Clin Risk Manag, 2015; 11, 45-51.
Sue, P. Humphrey, R. T. W. A review of saliva: Normal composition, flow, and function. The journal of prosthetic dentistry, 2001; 85, 162-169.
Niklander, S., Veas, L., Barrera, C., Fuentes, F., Chiappini, G., & Marshall, M. Risk factors, hyposalivation and impact of xerostomia on oral health-related quality of life. Brazilian Oral Research, 2017; 31.
Khovidhunkit, S. O., Suwantuntula, T., Thaweboon, S., Mitrirattanakul, S., Chomkhakhai, U., & Khovidhunkit, W. Xerostomia, hyposalivation, and oral microbiota in type 2 diabetic patients: a preliminary study. J Med Assoc Thai, 2009; 92(9), 1220-1228.
Cassolato, SF., Turnbull, RS. Xerostomia: clinical aspects and treatment. Gerodontology, 2003; 20(2), 64–77.
Villa A, Polimeni A, Strohmenger L, Cicciù D, Gherlone E, Abati S. Dental patients’ self-reports of xerostomia and associated risk factors. J Am Dent Assoc, 2011; 142(7), 811–816.
Ekström J, Khosravani N, Castagnola M, Messana I. Saliva and the control of its secretion. In: Ekberg O, editor. Dysphagia: Diagnosis and Treatment. Berlin: Springer-Verlag, 2012; 19–47.
Ship, J. A., Pillemer, S. R., & Baum, B. J. Xerostomia and the Geriatric Patient. Journal of the American Geriatrics Society, 2002; 50(3), 535-543.
Stack, K. M., & Papas, A. S. Xerostomia: Etiology and Clinical Management. Nutrition in Clinical Care, 2001; 4(1), 15-21.
Samnieng, P. Oral health status and treatment needs of elderly in phitsanulok. Naresuan University Journal, 2016; 24(1), 36-43.
Bardow, A., Nyvad, B., & Nauntofte, B. Relationships between medication intake, complaints of dry mouth, salivary flow rate and composition, and the rate of tooth demineralization in situ. Arch Oral Biol, 2001; 46(5), 413-423.
Pedersen AM, Bardow A, Jensen SB, Nauntofte B. Saliva and gastrointestinal functions of taste, mastication, swallowing and digestion. Oral Dis, 2002; 8(3):117–129.
Heintze, U., Birkhed D., Björn H. Secretion rate and buffer effect of resting and stimulated whole saliva as a function of age and sex. Swed Dent J, 1983; 7(6), 227–238.
Sreebny, LM, Vissink A. Dry Mouth: the malevolent symptom a clinical guide. Ames: Wiley-Blackwell; 2010.
Ericsson, Y. Clinical investigation of the salivary buffering action. Acta Odontal Scand, 1959; 17, 131-65.
Bradford, MM., A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal Biochem, 1976; 72, 248–254.
Ben Aryeh, H., Miron, D., Berdicevsky, I., Szargel, R., & Gutman, D. Xerostomia in the Elderly: Prevalence, Diagnosis, Complications and Treatment1. Gerodontology, 1985; 4(2), 77-82.
Tenovuo, J. Salivary parameters of relevance for assessing caries activity in individuals and populations. Community Dent Oral Epidemiol, 1997; 25, 82-86.
Farsi, N. M. Signs of oral dryness in relation to salivary flow rate, pH, buffering capacity and dry mouth complaints. BMC Oral Health, 2007; 7(1), 15. doi:10.1186/1472-6831-7-15.
Leal SC, Bittar J, Portugal A, Falcão DP, Faber J, Zanotta P. Medication in elderly people: its influence on salivary pattern, signs and symptoms of dry mouth. Gerodontology, 2010; 27(2),129-33.
Agha-Hosseini, F., Mirzaii-Dizgah, I., Moghaddam, P. P., & Akrad, Z. T. Stimulated whole salivary flow rate and composition in menopausal women with oral dryness feeling. Oral Dis, 2007; 13(3), 320-323.
Chaudhury, N. M., Shirlaw, P., Pramanik, R., Carpenter, G. H., & Proctor, G. B. Changes in Saliva Rheological Properties and Mucin Glycosylation in Dry Mouth. J Dent Res, 2015; 94(12), 1660-1667.
Mizuhashi, F., Koide, K., Toya, S., Takahashi, M., Mizuhashi, R., & Shimomura, H. Levels of the antimicrobial proteins lactoferrin and chromogranin in the saliva of individuals with oral dryness. Journal of Prosthetic Dentistry, 2015; 113(1), 35-38.
Ohyama, K., Moriyama, M., Hayashida, J. N., Tanaka, A., Maehara, T., Ieda, S.,Nakamura, S. Saliva as a potential tool for diagnosis of dry mouth including Sjogren's syndrome. Oral Dis, 2015; 21(2), 224-231.
Sharmila, B, Sangeeta, M, Rahul, K. Salivary pH: A diagnostic biomarker J Indian Soc Periodontol, 2013;17(4), 461–465.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2022 Naresuan Phayao Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยาไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย
The authors are themselves responsible for their contents. Signed articles may not always reflect the opinion of University of Phayao. The articles can be reproduced and reprinted, provided that permission is given by the authors and acknowledgement must be given.