
Predicting Factors of Symptoms among Persons Suspected of Acute Coronary Syndrome in Emergency Department, Secondary Hospital
Keywords:
Acute Coronary Syndrome, Emergency Department, Symptoms, Factors PredictingAbstract
This predictive correlational study aimed to identify factors that predict patient-reported symptoms of acute coronary syndrome (ACS) individuals presenting with suspected ACS at the emergency department of secondary hospital, A purposive sample of 419 individuals aged 35 years and older with suspected ACS was selected. Data were collected through interviews using a questionnaire, which included demographic information, a 15-symptom checklist, and a clinical data form. Descriptive statistics, Chi-Square, and binary logistic regression were employed for data analysis.
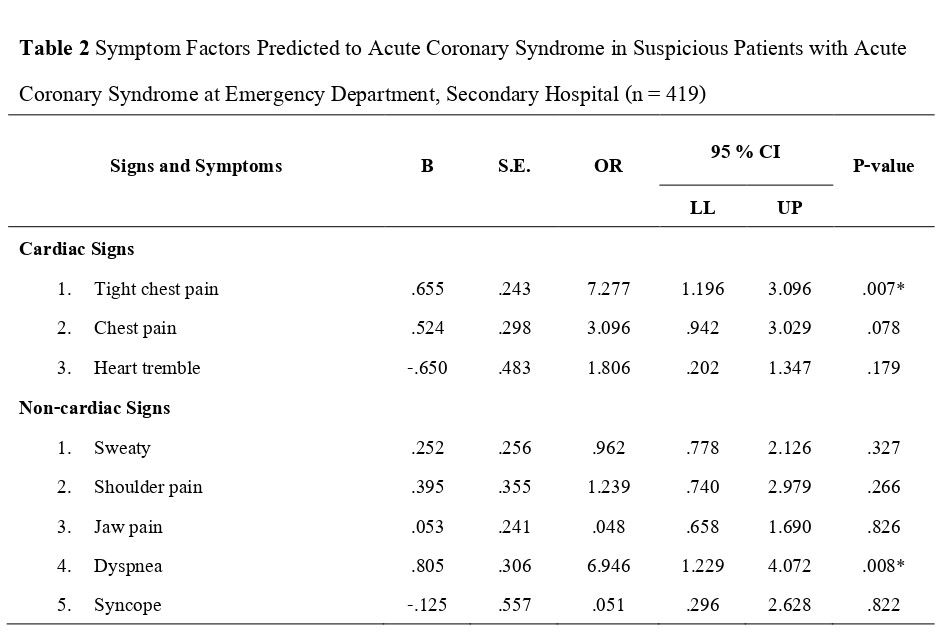
The results revealed that 62.53% of the participants developed ACS. Chest pain (OR=1.924, 95% CI 1.196–3.096, p=.007), shortness of breath (OR=2.237, 95% CI 1.229–4.072, p=.008), upper xiphoid and abdominal pain (OR=0.275, 95% CI 0.133–0.567, p<.001), and weakness or dizziness (OR=2.650, 95% CI 1.367–5.140, p=.004). Collectively, these factors predicted ACS with statistical significance at p <.05 and predicted the occurrence of ACS by 66.80%.
The findings suggest that healthcare providers should have prioritized early screening and monitoring of ACS, particularly in patients presenting with chest pain, shortness of breath, abdominal discomfort, and weakness or dizziness, to facilitate timely diagnosis, enhance treatment outcomes, and lower the risk of complications from delayed recognition.
References
Arora, G., & Bittner, V. (2017). Chest pain characteristics and sex in the early diagnosis of acute myocardial infarction. Current Cardiology Reports 2017, 17(2),5. http://doi.org/10.1007/ s11886-014-0557-5
Benjamin, E.J., Blaha, M.J., Chiuve, S.E., Cushman, M., Das, S.R., Deo R, Ferranti, M., Gillespie, C., Isas, C.R., Jiménez, M.C., Jordan, L.C., Judd, S. E, Lackland, L., Lichtman, H.L., Lisabeth, L, Liu, S., Longenecker, C.T., Mackey, R.H., Matsushita, K., ... Muntner, P. (2017). Heart disease and stroke statistics- 2017. Circulation, 135 (10), e146 - e603. http://doi.org/10.1161/ CIR.0000000000000485
Dodd, M., Janson, S., Facione, N., Facione, J., Froelicher, E. S., Humphreys, J., Kathryn, L., Miaskowski, C., Puntillo, K., Rankin, S., & Taylor, D. (2001). Advancing the science of symptom management. Journal of Advanced Nursing, 33(5), 668 - 676. http://doi.org/ 10.1046/j.1365-2648.2001. 01697.x
DeVon, H.A, Mirzaei, S., & Zègre‐Hemsey, J. (2020). Typical and Atypical Symptoms of Acute Coronary Syndrome: Time to Retire the Terms. Journal of the American Heart Association, 9 (7), 1 - 4. http://doi.org/org/10.1161/JAHA.119.015539
Emakhu, J., Monplaisir, L., Aguwa, C., Arslanturk, S., Masoud, S., Nassereddine, H., Hamam, S.M., & Miller, J.B. (2022). Acute coronary syndrome prediction in emergency care: A machine learning approach. Computer Methods and Programs in Biomedicine, 225. http://doi.org/ 10.1016/j.cmpb.2022.107080
Harris, J. K. (2021). Primer on binary logistic regression. Family Medicine and Community Health, 9(1), 1 - 17. https://doi.org/10.1136/fmch-2021-001290.
Karam, N., Bataille, S., Marijon, E., Giovannetti ,O., Tafflet, M., Savary, D, Benamer,H., Caussin,C., Garot,P., Juliard,J.M., Pires,v., Boche,T., Dupas,F., LeBail,G., Lamhaut,L., Laborne,F., Lefort,H., Mapouata,M., Lapostolle, F.,... Lambert,Y.(2016). Identifying patients at risk for prehospital sudden cardiac arrest at the early phase of myocardial infarction: The e-MUST study (evaluation en medecine d’urgence des strategies therapeutiques des infarctus du myocarde) AHAIASA Journals,134 (25). http://doi.org/ 10.1161/CIRCULATIONAHA. 116.022954
Medical Recoad Secondary Hospital (2023). Register of patients with Acute Coronary Syndrome Secondary Hospital 2023. Rasisalai Hospital, Sisaket Province.
Perona, M., Cooklin, A., Thorpe, C., O’Meara, P., & Rahman, A.M. (2024). Symptomology, Outcomes and Risk Factors of Acute Coronary Syndrome Presentations without Cardiac Chest Pain: A Scoping Review. European Cardiology Review,19, e12. http://doi.org/10. 15420/ecr.2023.45
Strategy and Planning Divistion. (2022, November 1). Public Health Statistics A.D. https://spd.moph. go.th/wp-content/uploads/2023/11/Hstatistic65.pdf
Supinski, D., Borg, B., Schmitz, K., Mullvain, R., Renier, C., & Benziger, C. (2021). Chest pain severity rating is a poor predictive tool in the diagnosis of ST-segment elevation myocardial infarction. Critical Pathways in Cardiology, 20(2),88 – 92. http://doi.org/org/10.1097/HPC. 000000 0000000241
Tae Du Jung (2022). A Brief Note on the Angina Pectoris and its Pathophysiology. Journal Clinical Experimemtal Cardiology 2022, 13(4), 1 - 10. http://doi.org/10.35248/2155-9880.22.13.725
Torres, M., & Moayedi, S. (2007). Evaluation of the acutely dyspneic elderly patient. Clinic in Geriatric Medicine, 23(2) , 307–325. http://doi.org/10.1016/j.cger.2007.01.007
World Health Organization. (2020, May 13 ) World Health Statistics 2020:Monitoring health for the SDGs, sustainable developmentgoals. https://www.who.int/publications/i/item/9789 240005105
Zègre-Hemsey, J.K., Burke, L.A., & DeVon, H.A. (2018). Patient-reported symptoms improve prediction of acute coronary syndrome in the emergency department. Research in Nursing and Health, 41(5), 459 – 468 http://doi.org/10.1002/nur.21902
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Princess of Naradhiwas University Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.


