
การพัฒนารูปแบบการเฝ้าระวังป้องกันการฆ่าตัวตายในผู้ป่วยโรคซึมเศร้า โรงพยาบาลกระแสสินธุ์
คำสำคัญ:
โรคซึมเศร้า, ฆ่าตัวตาย, การเฝ้าระวัง, การป้องกัน, การพัฒนารูปแบบบทคัดย่อ
ความเป็นมาและวัตถุประสงค์ การฆ่าตัวตายเป็นปัญหาสำคัญทางสาธารณสุข โดยเฉพาะ
ในผู้ป่วยโรคซึมเศร้าที่มีความเสี่ยงสูง การพัฒนารูปแบบการเฝ้าระวังป้องกันการฆ่าตัวตายที่เหมาะสมกับบริบทหน่วยบริการจึงมีความจำเป็น การศึกษานี้มีวัตถุประสงค์เพื่อศึกษาสภาพการณ์และปัจจัยที่มีผลต่อการฆ่าตัวตาย พัฒนารูปแบบการเฝ้าระวัง และประเมินประสิทธิผลของรูปแบบในผู้ป่วยโรคซึมเศร้า โรงพยาบาลกระแสสินธุ์
วิธีการวิจัย การวิจัยและพัฒนา แบ่งเป็น 3 ขั้นตอน 1) ศึกษาสภาพการณ์ ปัจจัยที่มีผลต่อการ
ฆ่าตัวตายและการเฝ้าระวังป้องกันการฆ่าตัวตาย โดยการสัมภาษณ์เชิงลึกในผู้ป่วยโรคซึมเศร้า อายุ 15 ปีขึ้นไป ที่มีประวัติพยายามฆ่าตัวตาย จำนวน 14 คน และการสนทนากลุ่มผู้ให้บริการสุขภาพจิต จำนวน 10 คน แพทย์ เภสัชกร พยาบาลวิชาชีพจิตเวช พยาบาลเยี่ยมบ้าน นักจิตวิทยา และพยาบาลผู้รับผิดชอบงานจิตเวชปฐมภูมิ 5 แห่ง 2) พัฒนารูปแบบการเฝ้าระวังป้องกันการฆ่าตัวตายจากการวิเคราะห์ข้อมูลเชิงคุณภาพ 3) ทดลองใช้และประเมินประสิทธิผลของรูปแบบในผู้ป่วยโรคซึมเศร้า จำนวน 34 คน เก็บข้อมูลก่อนและหลังการทดลองด้วยแบบคัดกรองโรคซึมเศร้า (9Q) แบบประเมินความเสี่ยงการ
ฆ่าตัวตาย (8Q) และแบบสอบถามพฤติกรรมป้องกันการฆ่าตัวตาย วิเคราะห์ข้อมูลด้วยสถิติ Paired Sample t-test และประเมินประโยชน์และคุณค่าของรูปแบบ
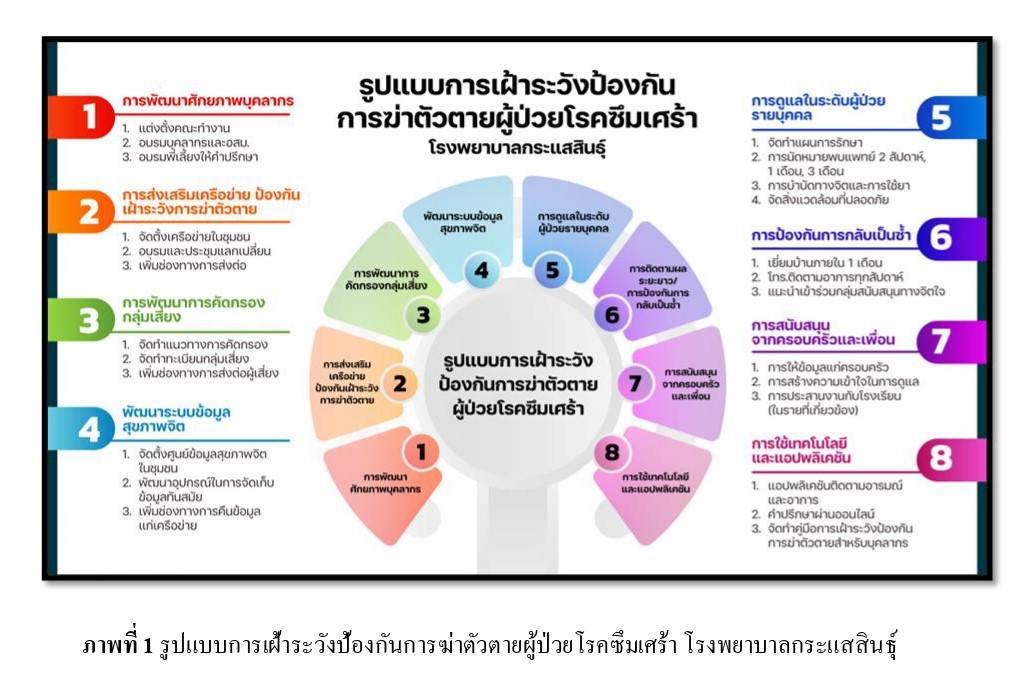
ผลการวิจัย พบว่า การคัดกรองและประเมินความเสี่ยงต่อการฆ่าตัวตายยังขาดความเป็นระบบ ปัจจัยที่มีผล ได้แก่ ปัจจัยส่วนบุคคล ประสบการณ์ สุขภาพ และสิ่งแวดล้อม รูปแบบช่วยพัฒนาศักยภาพบุคลากร คัดกรองกลุ่มเสี่ยง ส่งเสริมเครือข่ายครอบครัวและชุมชน จัดการข้อมูลสุขภาพจิต ดูแลรายบุคคล ติดตามป้องกันการกลับเป็นซ้ำ และใช้เทคโนโลยี หลังการนำรูปแบบไปใช้ พบว่า ภาวะซึมเศร้าลดลง จาก 2.68 ± 0.72 เป็น 0.52 ± 0.83, ความเสี่ยงต่อการฆ่าตัวตายลดลง จาก 1.59 ± 0.65 เป็น 0.38 ± 0.49 และ พฤติกรรมป้องกันการฆ่าตัวตายเพิ่มขึ้น จาก 77.32 ± 7.17 เป็น 86.21 ± 4.98
มีนัยสำคัญทางสถิติ (p < .001) รูปแบบมีประโยชน์ในการเฝ้าระวังอย่างเป็นระบบและเพิ่มความมั่นใจในการดูแลผู้ป่วยโรคซึมเศร้า
สรุปและข้อเสนอแนะ รูปแบบเหมาะสมกับบริบทโรงพยาบาลชุมชน มีประสิทธิภาพลดภาวะซึมเศร้า ความเสี่ยงต่อการฆ่าตัวตาย และเพิ่มพฤติกรรมป้องกัน ช่วยพัฒนาศักยภาพบุคลากร ติดตามผู้ป่วยรายบุคคล และส่งเสริมการมีส่วนร่วม ควรนำรูปแบบไปใช้ในการพัฒนาระบบบริการสุขภาพและชุมชน
เอกสารอ้างอิง
Arun, J. (2013). Biostatistics for health science research. Witthayaphat.
Berkman, L. F., & Glass, T. A. (2000). Social integration, social networks, social support, and health. In L. F. Berkman & I. Kawachi (Eds.), Social epidemiology (pp. 137–173). Oxford University Press.
Bohanna, I., & Wang, X. (2021). Suicide risk and prevention in patients with depression: Community-based interventions and follow-up care. International Journal of Mental Health, 50(2), 123 – 136. https://doi.org/10.1111/j.1753-6405.2012.00888.x
Buriram Hospital (2020). Annual report on mental health and suicide prevention among psychiatric patients and youth 2020. Author.
Cohen, J. (1977). Statistical power analysis for the behavioral sciences (Rev. ed.). Academic Press.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates.
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310–357. https://doi.org/10.1037/0033-2909.98.2.310
Crabtree, B. F., & Miller, W. L. (1992). Doing qualitative research. Sage Publications.
Department of Mental Health. (2022) (a). Community-based suicide prevention program for patients with depression. Ministry of Public Health.
Department of Mental Health. (2022) (b) Suicide situation report in Thailand. Ministry of Public Health.
Department of Mental Health. (2023). (a) Development of a suicide prevention surveillance model for patients with depression. Ministry of Public Health.
Department of Mental Health. (2023). (b) Situation and surveillance report on suicide in psychiatric and depressed patients. Ministry of Public Health.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175 – 191. https://doi.org/10.3758/BF03193146
Franklin, J. C., Ribeiro, J. D., Fox, K. R., Bentley, K. H., Kleiman, E. M., Huang, X., & Nock, M. K. (2022). Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychological Bulletin, 143(2), 187 – 232. https://doi.org/10.1037/bul0000346
Hawton, K., & Williams, K. (2022). Suicide prevention in healthcare settings: Gaps and challenges in community hospitals. The Lancet Psychiatry, 9(3), 123 – 135. https://doi.org/10.1016/S2215-0366(21)00466-4
Jirawattankul, A. (2013). Health science statistics for research. Vithayaphat Publishing.
Kanfer, F. H., & Gaelick-Buys, L. (1991). Self-management methods. In F. H. Kanfer & A. P. Goldstein (Eds.), Helping people change: A textbook of methods (4th ed., pp. 305–360). Pergamon Press.
Khammee, P., Punjaroen, S., Kongsuk, T., & Wannasinp, J. (2022). A study of risk and protective factors among suicide attempters in Health Region 7. Journal of Suicide Prevention of Thailand, 1(1), 15–28. https://doi.org/10.14456/jspt.2022.2
Krasaesin Hospital. (2023). Report on the suicide situation at Krasaesin Hospital, 2021–2023. Author.
National Health Commission Office. (2023). Mental health in adolescents: Stress, bullying, and depression. Author.
Phamarapa, N., Khammee, P., Tansri, P., & Kongsuk, T. (2022). Effectiveness of a suicide prevention and surveillance model for at-risk groups in the community. Journal of Psychiatric Nursing and Mental Health, 36(2), 45 – 60. https://he02.tci-thaijo.org/index.php/JPNMH
Phrommas, C., Khammee, P., Tansri, P., & Kongsuk, T. (2022). Accessibility of mental health services and support network building in rural communities: A case study of the Northeastern region. Journal of Health Science, 31(Suppl.), 112 – 125. https://thaidj.org/index.php/JHS
Regional Health Statistics Office 12 Songkhla. (2023). Suicide statistics in Health Region 12, Songkhla province: 2021–2023. Ministry of Public Health.
Sawat, P., Tansri, P., Khammee, P., Kongsuk, T., & Wannasinp, J. (2023). Development of a mental health support system in rural communities: Networking and access to services. Thai Journal of Mental Health, 31(2), 85 – 98. https://he01.tci-thaijo.org/index.php/TJMH
Tansri, P., Khammee, P., Kongsuk, T., Wannasinp, J., & Punjaroen, S. (2021). Evaluation of a community-based care and surveillance model for depressed patients to prevent suicide. Thai Journal of Mental Health, 29(3), 150 – 163. https://he01.tci-thaijo.org/index.php/TJMH
Turecki, G., Brent, D. A., Gunnell, D., O’Connor, R. C., & Pirkis, J. (2021). Suicide and suicide risk. Nature Reviews Disease Primers, 7, 1–26. https://doi.org/10.1038/s41572-021-00275-6
Waltz, C. F., Strickland, O. L., & Lenz, E. R. (2010). Measurement in nursing and health research (4th ed.). Springer Publishing Company.
World Health Organization. (2021). Suicide worldwide in the 21st century. Author.
World Health Organization. (2022). World suicide prevention report 2022: Mental health and suicide surveillance in the Western Pacific region. Author.
World Health Organization. (2023). Suicide worldwide in the 21st century: Global age-standardized suicide rates. Author.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2025 วารสารมหาวิทยาลัยนราธิวาสราชนครินทร์

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.


