Lung cancer screening in the population aged 55-75 years using low-dose computed tomography (LDCT) scan in Chiang Kham Hospital Phayao, Thailand: A Cross-Sectional Observational Pilot Study
Keywords:
Lung cancer screening, Chest x ray Artificial Intelligence, Low-dose computerized tomographyAbstract
This research was to survey the prevalence of lung cancer by screening with low-dose computerized tomography (LDCT) in high-risk populations and to study the factors associated with lung cancer. A cross-sectional observational pilot study was conducted in a sample of 100 Thai people who aged between 55 and 75 years-old in Chiang Kham District, Phayao Province, during August 3rd, 2024 - December 31th, 2024.
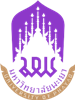
The instruments included a patient data record form and important risk factors, a digital chest X-ray (CXR AI) and a low-dose computed tomography (LDCT) result record form. We analyzed the relationship between high-risk LDCT results and other associated factors using multiple logistic regression, with statistical significance at p-value < 0.05. In the total of 100 samples, with an average age of 64 years–old, abnormal CXR AI readings were 72%. In the abnormal readings, 18% of them were lung nodules. In those lung nodule results, there was 14% of High Risk LDCT in Lung-RADS category 3 or higher. On the LDCT screening of the samples, the solid nodule was 75% of abnormal results. Most of the solid nodules were smaller than 8mm which were 36%.
A Multivariable logistic regression analysis showed the statistically significant related factor with high risk LDCT, specifically the volatile substances (OR 9.59, 95%CI 1.33-70.16, p = 0.02), alcoholic drinker (OR 7.73, 95% CI 0.86-69.63, p= 0.06) and old age (OR 1.16, 95% CI 0.99-1.35, p= 0.005). The use of CXR AI for initial screening increased the chance of detecting abnormal LDCT examination with Sensitivity Specificity 100% was 32.56%, NPV was 100%, and PPV was 19.44% respectively.
References
Siriwiwattnakul N. HOSPITAL-BASED CANCER REGISTRY 2022. Bangkok: National Cancer Institute; 2024. p.1-83.
Jayes L, Haslam PL, Gratziou CG, Powell P, Britton J, Vardavas C, et al. SmokeHaz: Systematic Reviews and Meta-analyses of the Effects of Smoking on Respiratory Health. Chest 2016;150(1):164-79.
Hill W, Lim LE, Weeden EC, Lee C, Augustine M, Chen K, et al. Lung adenocarcinoma promotion by air pollutants. Nature 2023;616(7955):159-67.
Rojanamatin J, Sangrajrang S, editors. Cancer in Thailand 2016-2018.10th ed. Bangkok: National Cancer Institute; 2021. p.1-170.
Bonney A, Malouf R, Marchal C, Manners D, Fong KM, Marshall HM, et al. Impact of low-dose computed tomography (LDCT) screening on lung cancer-related mortality. Cochrane Database Syst Rev 2022;8(8).
Tammemägi MC, Darling GE, Schmidt H, Walker MJ, Langer D, Leung YW, et al. Risk-based lung cancer screening performance in a universal healthcare setting. Nat Med 2024;30(4):1054-64.
Tammemägi MC. Selecting lung cancer screenees using risk prediction models-where do we go from here. Transl Lung Cancer Res 2018;7(3):243-53.
Tammemägi MC, Katki HA, Hocking WG, Church TR, Caporaso N, Kvale PA, et al. Selection criteria for lung-cancer screening. N Engl J Med 2013;368(8):728-36.
Marcus MW, Chen Y, Raji OY, Duffy SW, Field JK, et al. LLPi: Liverpool Lung Project Risk Prediction Model for Lung Cancer Incidence. Cancer Prev Res (Phila) 2015;8(6):570-5.
Sasieni D. editors. The Standard Protocol was developed by the NHS Cancer Programme with the CT Screening. 2nd ed. NHS England; 2022. p.1-40.
Lee JW, Kim HY, Goo JM, Kim EY, Lee SJ, Kim TJ, et al. Radiological Report of Pilot Study for the Korean Lung Cancer Screening (K-LUCAS) Project: Feasibility of Implementing Lung Imaging Reporting and Data System. Korean J Radiol 2018;19(4):803-8.
Triphuridet N, Singharuksa S, Vidhyakorn S. Practical difficulty of low dose computerized tomography as a lung cancer screening tool in an endemic area of tuberculosis. J Thorac Oncol 2017; 12(1): S568-S9.
Thai AA, Solomon BJ, Sequist LV, Gainor JF, Heist RS, et al. Lung cancer. Lancet 2021;398(10299):535-54.
Hussain MdS, Gupta G, Mishra R, Patel N, Gupta S, Alzarea SI, et al. Unlocking the secrets: Volatile Organic Compounds (VOCs) and their devastating effects on lung cancer. Pathol Res Pract 2024; 255:155-7.
Hamashima C. Cancer screening guidelines and policy making: 15 years of experience in cancer screening guideline development in Japan. Jpn J Clin Oncol. 2018;48(3):278-86.
Chutivanidchayakul F, Suwatanapongched T, Petnak T. Clinical and chest radiographic features of missed lung cancer and their association with patient outcomes. Clin Imaging 2023; 99:73-81.
Upaisilsathaporn P, Klawandee S, Wanchaijiraboon P. The Potential of Chest X-Ray Artificial Intelligence Detecting Missed Lung Cancer Diagnosis in a Community Based Cancer in Thailand.
J Thorac Oncol 2024; 19(10): S473-S74.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 University of Phayao

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยาไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย
The authors are themselves responsible for their contents. Signed articles may not always reflect the opinion of University of Phayao. The articles can be reproduced and reprinted, provided that permission is given by the authors and acknowledgement must be given.