Vernix in external ear canal: The manageable factor affecting newborn hearing screening results prior to hospital discharge
Keywords:
Newborn hearing screening, Vernix, Age, Otoacoustic emissionAbstract
Vernix obstruction in external ear canal leads to ineffective signal transmission between the equipment and inner ear during newborn hearing screening and contributes to a factor that cause false-positive result.
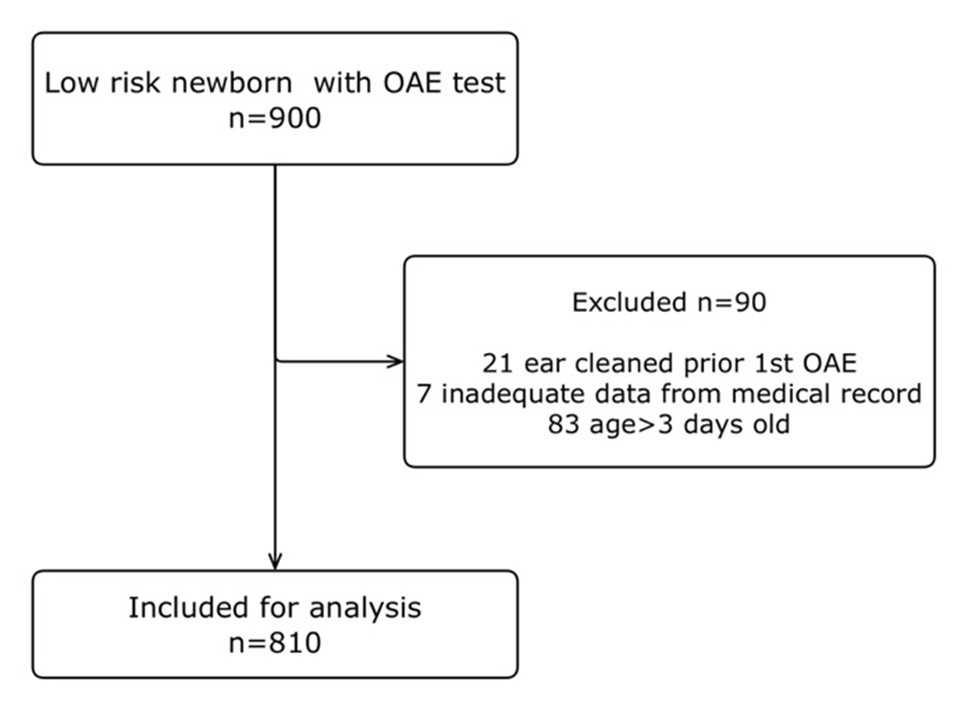
The retrospective chart review was conducted to compare referral rate in Otoacoustic emissions (OAE) testing between newborns prior vernix clearance and the same population after vernix clearance only in case of “Refer” result of low risk newborns aged 0-3 days old during hospital admission. 810 Newborns were recruited. Referral rate for initial OAE was 40.25% (326/810). This “Refer” group was sent to otolaryngologist for ear examination and vernix clearance if vernix obstruction was diagnosed. Referral rate after the clearance was 1.85% (15/810). 12 from 15 Newborns with “Refer” result proceeded the third test as OPD case. Referral rate of the third test is 0.12% (1/810). Referral rate of the newborns without cleaning of vernix (initial OAE) were decreased after vernix clearance significantly (P value <.00001) with odd ratio of 35.7. To conclude, vernix obstruction is important factor that cause false-positive result in OAE testing especially in early days of birth. Vernix clearance decreases referral rate significantly. Setting up the hearing screening program prior discharge that include vernix clearance in case of “Refer” result shows its effectiveness and could be considered to implement according to healthcare facilities’ circumstance.
References
Yimtae K, Pothaporn M, Kaewsiri S. Thailand’s Guidelines for Newborn Hearing Screening. 1st ed. Bangkok: Rajavithi Hospital; 2562. (in Thai)
Doyle KJ, Rodgers P, Fujikawa S, Newman E. External and middle ear effects on infant hearing screening test results. Otolaryngol Head Neck Surg 2000;122(4):477–81.
Chindavijak S, Tanamai N. Newborn Hearing Screening Service Guide. Rajavithi Hospital; 2563. 3–4 p. (in Thai)
Doyle KJ, Burggraaff B, Fujikawa S, Kim J, Macarthur CJ. Neonatal Hearing Screening with Otoscopy, Auditory Brain Stem Response, and Otoacoustic Emissions. Otolaryngol Head Neck Surg 1997 Jun;116(6):597–603.
Schwarz Y, Mauthner R, Kraus O, Gluk O, Globus O, Kariv L, et al. Newborn Hearing Screening: Early Ear Examination Improves the Pass Rate. J Int Adv Otol 2023;19(5):402–6.
Amphaiphan K, Thankham D. Pilot Implementation in Universal Newborn Hearing Screening Program in Buri Ram Hospital, Northeast Thailand. MJSBH 2023;38(1):33–42. (in Thai)
Shang Y, Hao W, Gao Z, Xu C, Ru Y, Ni D. An effective compromise between cost and referral rate: A sequential hearing screening protocol using TEOAEs and AABRs for healthy newborns. Int J Pediatr Otorhinolaryngol 2016;91:141–5.
Chindavijak S, Tanamai N, Khongsaksri A, Withyapraphaiphan S, Khitchaidiao A. Cost Effectiveness of Newborn Hearing Screening Protocol in Reduction of Refer Newborn Hearing Loss for Diagnosis. JDMS 2021;46(4):120–9. (in Thai)
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 University of Phayao

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยาไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย
The authors are themselves responsible for their contents. Signed articles may not always reflect the opinion of University of Phayao. The articles can be reproduced and reprinted, provided that permission is given by the authors and acknowledgement must be given.