ความชุกของภาวะมวลกล้ามเนื้อน้อยและความแข็งแรงของกล้ามเนื้อหายใจในผู้สูงอายุตั้งแต่ 65 ปี: การสำรวจเบื้องต้นแบบภาคตัดขวาง
คำสำคัญ:
ผู้สูงอายุ, ความแข็งแรงของกล้ามเนื้อหายใจ, ภาวะมวลกล้ามเนื้อน้อยบทคัดย่อ
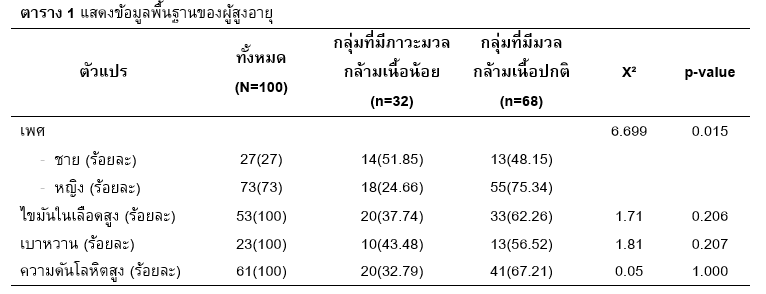
ผู้สูงอายุมีความเสี่ยงสูงในด้านของปัญหาสุขภาพ รวมถึงปัญหาทางด้านกล้ามเนื้อกระดูกและการหายใจ ปัจจุบันภาวะมวลกล้ามเนื้อน้อย (Sarcopenia) ซึ่งเป็นการสูญเสียมวลกล้ามเนื้อและสมรรถภาพร่างกาย โดยพบความสัมพันธ์กับการลดลงของสมรรถภาพทางกายรวมกับปัจจัยในการดำเนินชีวิตส่งผลต่อกิจกรรมในชีวิตประจำวัน และคุณภาพชีวิตที่ลดลง นอกจากนี้สมรรถภาพการหายใจที่ลดลงส่งผลให้เกิดความเสี่ยงต่อการภาวะแทรกซ้อนทางปอดในผู้สูงอายุ เช่นอาการหอบเหนื่อย ปอดอักเสบ เป็นต้น ดังนั้นจึงมีวัตถุประสงค์เพื่อการศึกษาความชุกของภาวะมวลกล้ามเนื้อน้อยและความแข็งแรงของกล้ามเนื้อหายใจในผู้สูงอายุ การศึกษานี้เป็นการสำรวจเบื้องต้นแบบภาคตัดขวาง โดยมีอาสาสมัครเป็นผู้สูงอายุตั้งแต่ 65 ปีขึ้นไป ทั้งหมด 100 คน อาสาสมัครทุกคนได้รับการคัดกรองภาวะมวลกล้ามเนื้อน้อยตามแนวทางของ Asian Working Group for Sarcopenia ฉบับปี 2019 ซึ่งมี 3 การทดสอบ คือ ความแข็งแรงของแรงบีบมือ ความเร็วในการดิน (ทดสอบด้วยระยะทางการเดิน 6 เมตร) และมวลกล้ามเนื้อ (ทดสอบด้วยเครื่องวัดองค์ประกอบของร่างกาย) และทดสอบความแข็งแรงของกล้ามเนื้อหายใจเข้า-ออก โดยใช้เครื่องวัดแรงดันของการหายใจ (Respiratory pressure meter) วิเคราะห์ข้อมูลด้วยสถิติเชิงพรรณนา การทดสอบความแตกต่างด้วยสถิติ t-test และ chi-square กำหนดนัยสำคัญทางสถิติ p-value < 0.05 โดยโปรแกรม SPSS version 23.0 จากการศึกษาพบความชุกของการเกิดภาวะมวลกล้ามเนื้อน้อยอยู่ที่ร้อยละ 32 พบผู้สูงอายุที่มีภาวะมวลกล้ามน้อยมีอายุมากกว่า (76.84 ± 7.33 เทียบ 71.15 ± 5.82, p<0.001) ความเร็วในการเดินลดลง (0.82 ± 0.19 เทียบ 1.05 ± 0.21 เมตรต่อวินาที, p<0.001) ดัชนีมวลกล้ามเนื้อน้อย (5.24 ± 0.90 เทียบ 7.46 ± 2.16 กิโลกรัมต่อตารางเมตร, p<0.001) และค่าความแข็งแรงกล้ามเนื้อหายใจเข้าสูงสุดน้อย (41.09 ± 23.08 เทียบ 59.77 ± 24.07 เซนติเมตรน้ำ, p<0.001) เมื่อเทียบกับกลุ่มมีภาวะมวลกล้ามเนื้อปกติ ดังนั้นในการศึกษานี้พบผู้สูงอายุตั้งแต่ 65 ปีขึ้นไปมีความชุกของการเกิดอยู่ที่ร้อยละ 32 ทั้งนี้ผู้สูงอายุส่วนใหญ่มีความแข็งแรงกล้ามเนื้อลดลงโดยผู้สูงอายุที่มีภาวะมวลกล้ามเนื้อน้อยพบความแข็งแรงกล้ามเนื้อหายใจเข้าน้อยกว่าผู้สูงอายุที่มีมวลกล้ามเนื้อปกติ
เอกสารอ้างอิง
Keller K. Sarcopenia. Wiener Medizinische Wochenschrift. 2019;169(7):157-72.
Larsson L, Degens H, Li M, Salviati L, Lee Yi, Thompson W, et al. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiological Reviews. 2018;99(1):427-511.
Nagano A, Wakabayashi H, Maeda K, Kokura Y, Miyazaki S, Mori T, et al. Respiratory Sarcopenia and Sarcopenic Respiratory Disability: Concepts, Diagnosis, and Treatment. The journal of nutrition, health & aging. 2021;25(4):507-15.
Shin HI, Kim D-K, Seo KM, Kang SH, Lee SY, Son S. Relation Between Respiratory Muscle Strength and Skeletal Muscle Mass and Hand Grip Strength in the Healthy Elderly. Ann Rehabil Med. 2017;41(4):686-92.
Lowery EM, Brubaker AL, Kuhlmann E, Kovacs EJ. The aging lung. Clinical interventions in aging. 2013;8:1489-96.
Bordoni B, Morabito B, Simonelli M. Ageing of the Diaphragm Muscle. Cureus. 2020;12(1):e6645.
Jones TE, Stephenson KW, King JG, Knight KR, Marshall TL, Scott WB. Sarcopenia--mechanisms and treatments. Journal of geriatric physical therapy (2001).
;32(2):83-9.
Waters DL, Mullins PG, Qualls CR, Raj DS, Gasparovic C, Baumgartner RN. Mitochondrial function in physically active elders with sarcopenia. Mechanisms of ageing and development. 2009;130(5):315-9.
Morisawa T, Kunieda Y, Koyama S, Suzuki M, Takahashi Y, Takakura T, et al. The Relationship between Sarcopenia and Respiratory Muscle Weakness in Community-Dwelling Older Adults. International journal of environmental research and public health. 2021;18(24).
Shafiee G, Keshtkar A, Soltani A, Ahadi Z, Larijani B, Heshmat R. Prevalence of sarcopenia in the world: a systematic review and meta- analysis of general population studies. Journal of Diabetes & Metabolic Disorders. 2017;16(1):21.
Petermann-Rocha F, Balntzi V, Gray SR, Lara J, Ho FK, Pell JP, et al. Global prevalence of sarcopenia and severe sarcopenia: a systematic review and meta-analysis. Journal of cachexia, sarcopenia and muscle. 2022;13(1):86-99.
Yuenyongchaiwat K, Boonsinsukh R. Sarcopenia and Its Relationships with Depression, Cognition, and Physical Activity in Thai Community-Dwelling Older Adults. Current Gerontology and Geriatrics Research. 2020;2020:8041489.
Chen LK, Woo J, Assantachai P, Auyeung TW, Chou MY, Iijima K, et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. Journal of the American Medical Directors Association. 2020;21(3):300-7.e2.
ATS/ERS Statement on respiratory muscle testing. Am J Respir Crit Care Med. 2002;166(4):518-624.
Makizako H, Nakai Y, Tomioka K, Taniguchi Y. Prevalence of sarcopenia defined using the Asia Working Group for Sarcopenia criteria in Japanese community-dwelling older adults: A systematic review and meta-analysis. Physical Therapy Research. 2019;22(2):53-7.
Ohara DG, Pegorari MS, Oliveira dos Santos NL, de Fátima Ribeiro Silva C, Monteiro RL, Matos AP, et al. Respiratory Muscle Strength as a Discriminator of Sarcopenia in Community-Dwelling Elderly: A Cross-Sectional Study. The journal of nutrition, health & aging. 2018;22(8):952-8.
Cruz-Jentoft AJ, Sayer AA. Sarcopenia. The Lancet. 2019;393(10191):2636-46.
Dhillon RJ, Hasni S. Pathogenesis and Management of Sarcopenia. Clinics in geriatric medicine. 2017;33(1):17-26.
Templeman L, Roberts F. Effectiveness of expiratory muscle strength training on expiratory strength, pulmonary function and cough in the adult population: a systematic review. Physiotherapy. 2020;106:43-51.
Kendall F, Oliveira J, Peleteiro B, Pinho P, Bastos PT. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: a systematic review and meta-analysis. Disability and rehabilitation. 2018;40(8):864-82.
Nepomuceno BRV, Barreto MdS, Almeida NC, Guerreiro CF, Xavier-Souza E, Neto MG. Safety and efficacy of inspiratory muscle training for preventing adverse outcomes in patients at risk of prolonged hospitalisation. Trials. 2017;18(1):626.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2023 มหาวิทยาลัยพะเยา

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยา ไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย