ปัจจัยเสี่ยงของการเกิดภาวะลำไส้อักเสบชนิดเนื้อตายในทารกน้ำหนักตัวน้อยมาก ในโรงพยาบาลหนองคาย
คำสำคัญ:
ภาวะลำไส้อักเสบชนิดเนื้อตาย, ทารกคลอดก่อนกำหนด, ทารกน้ำหนักตัวน้อยมากบทคัดย่อ
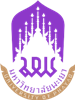
ภาวะลำไส้อักเสบชนิดเนื้อตายเป็นปัญหาระบบทางเดินอาหารที่สำคัญและเป็นภาวะฉุกเฉินของระบบทางเดินอาหารที่พบได้บ่อยที่สุดในทารกเกิดก่อนกําหนด อุบัติการณ์แตกต่างกันตามเชื้อชาติ พบว่าปัจจัยเสี่ยงที่มีอิทธิพลมากที่สุดต่อการเกิดภาวะลำไส้อักเสบชนิดเนื้อตายคือ การเกิดก่อนกําหนดและทารกน้ำหนักตัวน้อย ในขณะที่หลายการศึกษา พบว่าปัจจัยร่วมที่สําคัญ ได้แก่ การขาดออกซิเจนในระยะปริกําเนิด การให้นมผสมผ่านทางเดินอาหาร การหยุดหายใจ การใส่สายสวนหลอดเลือด ภาวะเลือดข้น การศึกษานี้จึงมีวัตถุประสงค์เพื่อศึกษาปัจจัยเสี่ยงของการเกิดภาวะลำไส้อักเสบชนิดเนื้อตายในทารกน้ำหนักตัวน้อยมาก (น้ำหนักแรกเกิดน้อยกว่า 1,500 กรัม) ที่เข้ารับการรักษาในหอผู้ป่วยทารกแรกเกิดวิกฤต โรงพยาบาลหนองคาย วิเคราะห์ปัจจัยต่างๆโดยใช้สถิติ Univariate analysis แล้วนำเฉพาะปัจจัยที่ p<0.20 มาวิเคราะห์ต่อโดยใช้สถิติ Multivariate logistic regression มีนัยสำคัญทางสถิติที่ p<0.05 จํานวนกลุ่มตัวอย่างที่ศึกษาในครั้งนี้ 167 ราย มีภาวะลำไส้อักเสบชนิดเนื้อตาย 25 ราย เมื่อวิเคราะห์ข้อมูลโดยใช้สถิติ Univariate analysis พบว่ามีปัจจัยเสี่ยงของการเกิดภาวะลำไส้อักเสบชนิดเนื้อตายในทารกน้ำหนักตัว
น้อยมาก 7 ปัจจัยคือ ภาวะน้ำคร่ำแตกก่อนการเจ็บครรภ์คลอด ภาวะติดเชื้อในกระแสเลือด ภาวะปอดอักเสบจากการใช้เครื่องช่วยหายใจ การใส่สายสวนหลอดเลือดแดงสะดือ การได้รับเลือด การใช้เครื่องช่วยหายใจ และภาวะเส้นเลือดหัวใจเกิน และเมื่อนำปัจจัยต่างๆเหล่านี้มาวิเคราะห์ต่อโดยใช้สถิติ Multivariate logistic regression พบว่ามีเพียงปัจจัยเดียวที่มีนัยสำคัญทางสถิติคือ การได้รับเลือด (adjusted OR 6.13, 95% CI : 1.23–30.47, p=0.01) ดังนั้นจึงควรประเมินความจำเป็นของการให้เลือดในทารกน้ำหนักตัวน้อยมากอย่างเคร่งครัด และติดตามอาการของภาวะลำไส้อักเสบชนิดเนื้อตายอย่างใกล้ชิดหลังได้รับเลือดหรือส่วนประกอบของเลือดทุกครั้ง
เอกสารอ้างอิง
Llanos AR, Moss ME, Pinzòn MC, Dye T, Sinkin RA, Kendig JW. Epidemiology of neonatal necrotizing enterocolitis: a population-based study. Paediatr Perinat Epidemiol. 2002;16(4):342-9.
Holman RC, Stoll BJ, Curns AT, Yorita KL, Steiner CA, Schonberger LB. Necrotizing enterocolitis hospitalizations among neonates in the United States. Paediatr Perinat Epidemiol. 2006;20(6):498-506.
Sankaran K, Puckett B, Lee DS, Seshia M, Boulton J, Qiu Z, Lee SK; Variations in incidence of necrotizing enterocolitis in Canadian neonatal intensive care units. J Pediatr Gastroenterol Nutr. 2004;39(4):366-72.
Yee WH, Soraisham AS, Shah VS, Aziz K, Yoon W, Lee SK, et al. Incidence and timing of presentation of necrotizing enterocolitis in preterm infants. Pediatrics. 2012;129(2):e298-304.
Gephart SM, McGrath JM, Effken JA, Halpern MD. Necrotizing Enterocolitis Risk. Adv Neonatal Care. 2012;12:77-89.
Llanos AR, Moss ME, Pinzòn MC, Dye T, Sinkin RA, Kendig JW. Epidemiology of neonatal necrotizing enterocolitis: a population-based study. Paediatr Perinat Epidemiol. 2002;16(4):342-9.
Carter BM, Diane Davis H, FAAN, Tanaka D, Schwartz T. The relationship between black race, Maternal infection and NEC in the preterm infant. Newborn and Infant Nursing Reviews. 2013;13(4):166-170.
Dominguez KM, Moss RL. Necrotizing enterocolitis. Clin Perinatol. 2012;39(2):387-401.
Fox TP, Godavitarne C. What really causes necrotizing enterocolitis?. ISRN Gastroenterol. 2012:2012;628317. doi: 10.5402/2012/628317.
Samuels N, van de Graaf RA, de Jonge RCJ, Reiss IKM, Vermeulen MJ. Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr. 2017;17(1):105.
Lu CY, Liu KF, Qiao GX, Luo Y, Cheng HQ, DU SZ. Risk factors for necrotizing enterocolitis in preterm infants: a Meta analysis. Zhongguo Dang Dai Er Ke Za Zhi. 2022;24(8):908-916.
Sangkhathat S, Kunapermsiri T, Leksrisakun P, Laohapensang M. Gastric perforation in very low birth weight infants following indomethacin administration: 2 case reports. Siriraj Hosp Gaz. 2000;52(7):492-496.
Berman L, Moss RL. Necrotizing enterocolitis: an update. Semin Fetal Neonatal Med. 2011; 16(3):145-50.
Alsaied A, Islam N, Thalib L. Global incidence of Necrotizing Enterocolitis: a systematic review and Meta-analysis. BMC Pediatr. 2020;20(1):344.
Walsh MC, Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am. 1986;33(1):179-201.
Stout G, Lambert DK, Baer VL, Gordon PV, Henry E, Wiedmeier SE, et al. Necrotizing enterocolitis during the first week of life: a multicentered case-control and cohort comparison study. J Perinatol. 2008;28(8):556-60.
Patel RM, Knezevic A, Shenvi N, Hinkes M, Keene S, Roback JD, et al. Association of red blood cell transfusion, anemia, and necrotizing enterocolitis in very low-birth-weight infants. JAMA. 2016;315(9):889-97. DOI: 10.1001/jama.2016.1204.
MohanKumar K, Namachivayam K, Song T, Cha JB, Slate A, Hendrickson JE, et al. A murine neonatal model of necrotizing enterocolitis caused by anemia and red blood cell transfusions. Nat Commun. 2019;10(1):3494 DOI: 10.1038/s41467-019-11199-5.
Gordon PV, Swanson JR, Attridge JT, Clark R. Emerging trends in acquired neonatal intestinal disease: Is it time to abandon Bell’s criteria?. J Perinatol. 2007;27(11):661-71. DOI: 10.1038/sj.jp.7211782.
Been JV, Lievense S, Zimmermann LJ, Kramer BW, Wolfs TG. Chorioamnionitis as a risk factor for necrotizing enterocolitis: a systematic review and meta-analysis. J Pediatr. 2013;162(2):236–242.
Gunasekaran V, Rodriguez RJ, Porcelli P, Jawale N, Shenberger J, Garg PM. Clinical impact of the PDA and its management on outcomes of preterm infants with NEC: A review. Am J Perinatol. 2025;10 10.1055/a-2685-2169. doi: 10.1055/a-2685-2169.
Khashu M, Dame C, Lavoie PM, De Plaen IG, Garg PM, Sampath V, et al. Current Understanding of Transfusion-associated Necrotizing Enterocolitis: Review of Clinical and Experimental Studies and a Call for More Definitive Evidence. Newborn (Clarksville). 2022;1(1):201-8.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2025 มหาวิทยาลัยพะเยา

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
ผู้นิพนธ์ต้องรับผิดชอบข้อความในบทนิพนธ์ของตน มหาวิทยาลัยพะเยา ไม่จำเป็นต้องเห็นด้วยกับบทความที่ตีพิมพ์เสมอไป ผู้สนใจสามารถคัดลอก และนำไปใช้ได้ แต่จะต้องขออนุมัติเจ้าของ และได้รับการอนุมัติเป็นลายลักษณ์อักษรก่อน พร้อมกับมีการอ้างอิงและกล่าวคำขอบคุณให้ถูกต้องด้วย